
Summary of Ebola talk
Thanks Eimhear for a comprehensive review of recent updates on Ebola.
Today the WHO has predicted a worse case scenario of up to 20000 cases before the end of this epidemic is brought undercontrol (hopefully by the middle of next year) .The BBC reports that it is thought that the actual number of cases may be 4 x the advertised 3000 . The measures needed to control the outbreak will cost 500 million dollars and will involve 175 international case workes and more than 10 thousands national workers
current quick glance guidelines/ algorithm are available via the HSE website here
Precautions involve using personal protective gear ( Face mask , water proof gown, gloves over gown , closed shoes , eye shied ) . Although no droplet spread as such , infection occurs when there is close contact with bodily fluids ( semen , saliva , faecies , blood.) it appears that this fluid must come into contact with mucosa or broken skin. The virus can survive for many months in body secretions. Health workers within one metre contact are at risk unless full PPE is used
In our institution the current hospital protocol is that a patient that has any risk should be transported from triage to AAU ( with personel using PPE ) . The triage room should then be disinfected ( standard chlorhexidine etc)
Currently our ED is not equipped to handle suspected cases
Thanks also to Marcus Chou ( ENT consultant) for part one of ENT review – Epistaxis
To summarise
-epistaxis is common ( exact prevalence uncertain because it is mostly self limiting at home). Ninety percent idiopathic
– the management of epistaxis is the responsibility of ED until ENT takes over.
– ED may end up being responsible for the active treatment and resuscitation right up until the unstable patient is taken to theatre by ENT
Some of the essential equipment in ed must include
Head light source ( unless you have three hands)
Nasal speculum – do ed doctors really know how to hold a nasal speculum?

ENT suction

Co phenylcaine

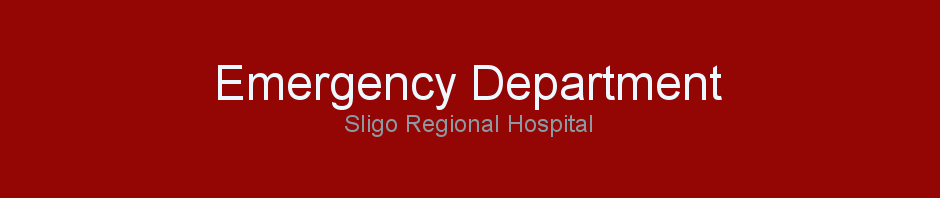
Appropriate packing – rapid rhino > merocel
Alternatives include ………
Silvernitrite sticks ( remember you just apply DRY for a second or two – to avoid septal perforation or unsightly staining of skin)
Approach
ED doctors know how to resuscitate ( I hope) – access/ airway / opiate analgesia prn/ monitoring
Remove clot with suction
apply cophenylcaine ( 120 euros per bottle )
use cotton wool or plegets as an added measure these can be soaked in cophenylcaine
visualize littles area
cauterise culprit vessel with care
pack with rapid rhino if this fails
pack ohter side with rapid rhino if this fails
take out and use standard packing if this fails – patient will not be liking this !
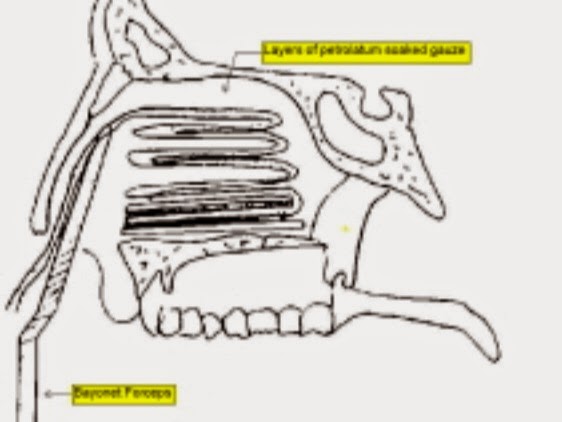
posterior bleeds are uncommon < 5 percent and are treated with tampnade ( ie a Foley catheter baloon to seal off the posteior part of nasal cavity in conjunction with packing and forceps at nose to hold taught – these patients will need to go to theatre and all patients will need ENT admission – current dogma recommends that packs stay in for three days and that antibiotics are given



Good session today, guys. You can find out the up-to-date information on Ebola on the HPSC website here.